America is Failing its Black Mothers

Serena Williams knew her body well enough to listen when it told her something was wrong. Winner of 23 Grand Slam singles titles, she’d been playing tennis since age 3—as a professional since 14. Along the way, she’d survived a life-threatening blood clot in her lungs, bounced back from knee injuries, and drowned out the voices of sports commentators and fans who criticized her body and spewed racist epithets. At 36, Williams was as powerful as ever. She could still devastate opponents with the power of a serve once clocked at 128.6 miles per hour. But in September 2017, on the day after delivering her baby, Olympia, by emergency C-section, Williams lost her breath and recognized the warning signs of a serious condition.
She walked out of her hospital room and approached a nurse, Williams later told Vogue magazine. Gasping out her words, she said that she feared another blood clot and needed a CT scan and an IV of heparin, a blood thinner. The nurse suggested that Williams’ pain medication must be making her confused. Williams insisted that something was wrong, and a test was ordered—an ultrasound on her legs to address swelling. When that turned up nothing, she was finally sent for the lung CT. It found several blood clots. And, just as Williams had suggested, heparin did the trick. She told Vogue, “I was like, listen to Dr. Williams!”
But her ordeal wasn’t over. Severe coughing had opened her C-section incision, and a subsequent surgery revealed a hemorrhage at that site. When Williams was finally released from the hospital, she was confined to her bed for six weeks.
[contentarea class=”bwh-big-img”]

Wanda Irving holds her granddaughter, Soleil, in front of a portrait of Soleil’s mother, Shalon Irving, at home in Sandy Springs, Georgia. Wanda has been raising Soleil since Shalon—an epidemiologist with the U.S. Centers for Disease Control and Prevention—died in 2017 from complications of hypertension a few weeks after giving birth.
[/contentarea]
Like Williams, Shalon Irving, an African American woman, was 36 when she had her baby in 2017. An epidemiologist at the U.S. Centers for Disease Control and Prevention (CDC), she wrote in her Twitter bio, “I see inequity wherever it exists, call it by name, and work to eliminate it.”
Irving knew her pregnancy was risky. She had a clotting disorder and a history of high blood pressure, but she also had access to top-quality care and a strong support system of family and friends. She was doing so well after the C-section birth of her baby, Soleil, that her doctors consented to her request to leave the hospital after just two nights (three or four is typical). But after she returned home, things quickly went downhill.
For the next three weeks, Irving made visit after visit to her primary care providers, first for a painful hematoma (blood trapped under layers of healing skin) at her incision, then for spiking blood pressure, headaches and blurred vision, swelling legs, and rapid weight gain. Her mother told ProPublica that at these appointments, clinicians repeatedly assured Irving that the symptoms were normal. She just needed to wait it out. But hours after her last medical appointment, Irving took a newly prescribed blood pressure medication, collapsed, and died soon after at the hospital when her family removed her from life support.
[sidebar position=”right” class=”bwh-sb”]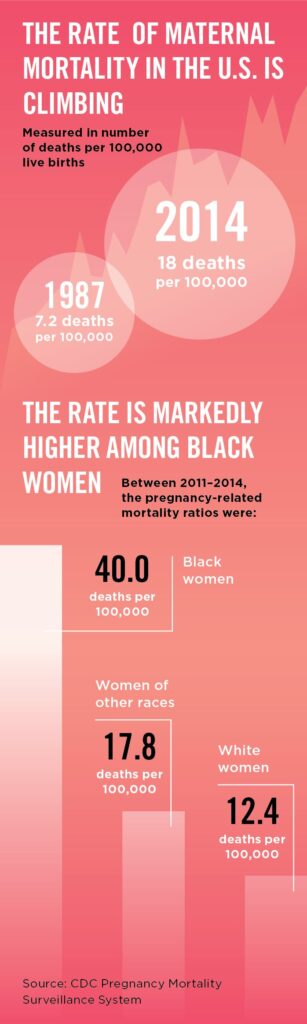 [/sidebar]
[/sidebar]
Viewed up close, the deaths of mothers like Irving are devastating, private tragedies. But pull back, and a picture emerges of a public health crisis that’s been hiding in plain sight for the last 30 years.
Following decades of decline, maternal deaths began to rise in the United States around 1990—a significant departure from the world’s other affluent countries. By 2013, rates had more than doubled. The CDC now estimates that 700 to 900 new and expectant mothers die in the U.S. each year, and an additional 500,000 women experience life-threatening postpartum complications. More than half of these deaths and near deaths are from preventable causes, and a disproportionate number of the women suffering are black.
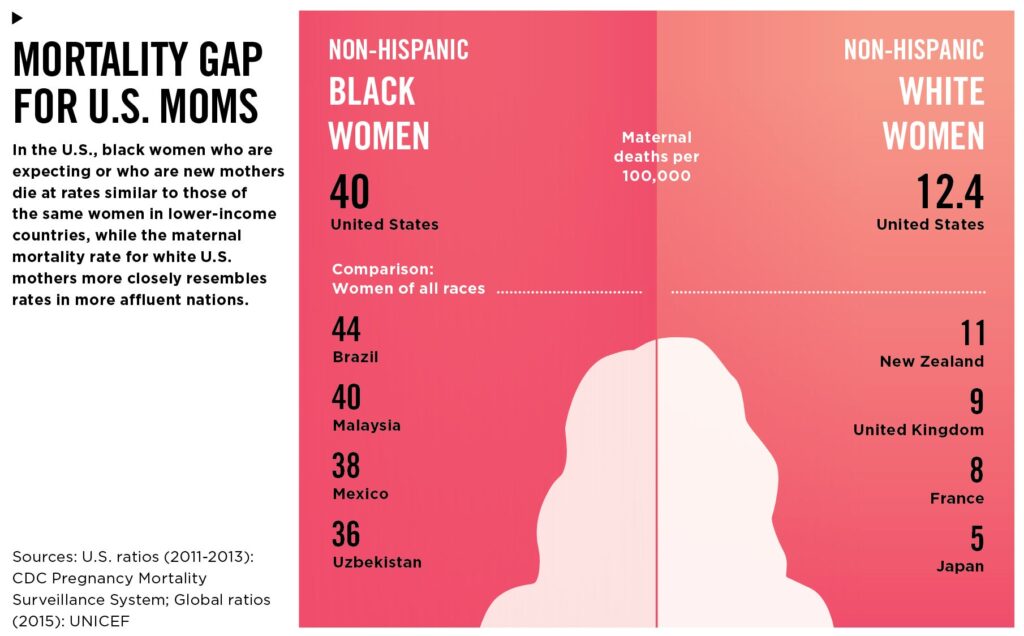
Put simply, for black women far more than for white women, giving birth can amount to a death sentence. African American women are three to four times more likely to die during or after delivery than are white women. According to the World Health Organization, their odds of surviving childbirth are comparable to those of women in countries such as Mexico and Uzbekistan, where significant proportions of the population live in poverty.
Irving’s friend Raegan McDonald-Mosley, chief medical director for Planned Parenthood Federation of America, told ProPublica, “You can’t educate your way out of this problem. You can’t health-care-access your way out of this problem. There’s something inherently wrong with the system that’s not valuing the lives of black women equally to white women.”
Lost mothers
Speaking at a symposium hosted by the Maternal Health Task Force at the Harvard T.H. Chan School of Public Health in September 2018, investigative reporter Nina Martin noted telling commonalities in the stories she’s gathered about mothers who died. Once a baby is born, he or she becomes the focus of medical attention. Mothers are monitored less, their concerns are often dismissed, and they tend to be sent home without adequate information about potentially concerning symptoms. For African American mothers, the risks jump at each stage of the labor, delivery, and postpartum process.
Neel Shah, an obstetrician-gynecologist at Beth Israel Deaconess Medical Center in Boston and director of the Delivery Decisions Initiative at Ariadne Labs, recalls being struck by Martin’s ProPublica-NPR series Lost Mothers, which delved into the issue. “The common thread is that when black women expressed concern about their symptoms, clinicians were more delayed and seemed to believe them less,” he says. “It’s forced me to think more deeply about my own approach. There is a very fine line between clinical intuition and unconscious bias.”
For members of the public, the experiences of prominent black women may prove to be a teachable moment. When pop superstar Beyoncé developed the hypertensive disorder pre-eclampsia—which left untreated can kill a mother and her baby—after delivering her twins by emergency C-section in 2017, Google searches related to the condition spiked. According to the U.S. Agency for Healthcare Research and Quality, pre-eclampsia—one of the leading causes of maternal death—and eclampsia (seizures that develop after pre-eclampsia) are 60 percent more common in African American women than in white women, and also more severe. If it can happen to Beyoncé—an international star who presumably can afford the highest-quality medical care—it can happen to anyone.
Weathering report
Arline Geronimus, SD ’85, has been talking about the effects of racism on health for decades, even when others haven’t wanted to listen. Growing up in the 1960s in Brookline, Massachusetts, Geronimus, who is white, absorbed the messages of the Civil Rights movement and the harrowing stories of her Jewish family’s experiences in czarist Russia. When she headed off to Princeton as an undergraduate, she resolved to find a way to fight against injustice. Her initial plan to become a civil rights lawyer gave way when she discovered the power and potential of public health research.
Geronimus worked as a research assistant for a professor studying teen pregnancy among poor urban residents, and, as a volunteer at a Planned Parenthood clinic, witnessed close-up the lives of pregnant black teens living in poverty in Trenton, New Jersey. She felt a chasm open up between what some of her white male professors were confidently explicating about the lives of these adolescents and how the young women themselves saw their lives.

Arline Geronimus, SD ’85
According to the conventional wisdom at the time, Geronimus says, teen pregnancy was the primary driver of maternal and infant deaths and a host of multigenerational health and social problems among low-income African Americans. Researchers focused on this issue while ignoring broader systemic factors.
Geronimus sought to connect the dots between the health problems the girls experienced, like asthma and type 2 diabetes, and negative forces in their lives. She visited them in their crumbling apartments and accompanied them to medical appointments where doctors treated the girls like props, without agency in their own care. And she noticed that they seemed older, somehow, than girls the same age whom Geronimus knew.
“That’s when I got the fire in my belly,” she says, her voice rising. “These young women had real, immediate needs that those of us in the hallowed halls of Princeton could have helped address. But we weren’t seeing those urgent needs. We just wanted to teach them about contraception.”
Geronimus came to the Harvard Chan School to learn how to rigorously explore the ways that social disadvantage corrodes health—a concept for which she coined the term “weathering.” Her adviser, Steven Gortmaker, professor of the practice of health sociology, provided data for her to correlate infant mortality by maternal age. While most such studies put mothers into broad categories of teen and not-teen, Geronimus looked at the risks they faced at every age. The results were surprising even to her.
White women in their 20s were more likely to give birth to a healthy baby than those in their teens. But among black women, the opposite was true: The older the mother, the greater the risk of maternal and newborn health complications and death. In public health, the condition of a baby is considered a reliable proxy for the health of the mother. Geronimus’ data suggested that black women may be less healthy at 25 than at 17.
“Being able to see those stark numbers was essential for me,” says Geronimus, who is now a professor of health behavior and health education at the University of Michigan School of Public Health and a member of the National Academy of Medicine. And the implications were staggering. If young black women were already showing signs of weathering, how would that play out over the rest of their lives—and what could be done to stop it?
Geronimus’ questions were ahead of their time. The press and the public—even other scientists—misinterpreted her findings as a recommendation that black women have children in their teens, she says, recalling with a sigh such clueless headlines as, “Researcher says let them have babies.”
In the 1970s, even researchers who broached the topic of racial differences in health outcomes—and few did—focused on small pieces of the puzzle. Some were looking at genetics, others at behavioral and cultural differences or health care access. “No one wanted to look at what was wrong with how our society works and how that can be expressed in the health of different groups,” Geronimus says. Over time, her ideas would become harder to dismiss.
The tide began to turn in the early 1980s, when former Health and Human Services Secretary Margaret Heckler convened the first group of experts to conduct a comprehensive study of the health status of minority populations. As the field of social epidemiology took off, the Report of the Secretary’s Task Force on Black and Minority Health (also known as the Heckler Report) brought Geronimus’ animating questions into mainstream debate.
Then, in 1993, researchers identified a physiological mechanism that could finally explain weathering: allostatic load. “We as a species are designed to respond to threats to life by having a physiological stress response,” Geronimus explains. “When you face a literal life-or-death threat, there is a short window of time during which you must escape or be killed by the predator.” Stress hormones cascade through the body, sending blood flowing to the muscles and the heart to help the body run faster and fight harder. Molecules called pro-inflammatory cytokines are produced to help heal any wounds that result.
These processes siphon energy from other bodily systems that aren’t enlisted in the fight-or-flight response, including those that support healthy pregnancies. That’s not important if the threat is short term, because the body’s biochemical homeostasis quickly returns to normal. But for people who face chronic threats and hardships—like struggling to make ends meet on a minimum wage job or witnessing racialized police brutality—the fight-or-flight response may never abate. “It’s like facing tigers coming from several directions every day,” Geronimus says, and the damage is compounded over time.
As a result, health risks rise at increasingly younger ages for chronic conditions like hypertension and type 2 diabetes. Depression and sleep deprivation become more common. People are also more likely to engage in risky coping behaviors, such as overeating, drinking, and smoking.
Geronimus’ foundational work in the 1980s and 1990s has been cited by David R. Williams, the Florence Sprague Norman and Laura Smart Norman Professor of Public Health at the Harvard Chan School, an internationally recognized expert in the ways that racism and other social influences affect health. His Everyday Discrimination Scale is one of the most widely used measures of discrimination in health studies. It includes questions that measure experiences such as being treated with discourtesy, receiving poorer service than others in restaurants or stores, or witnessing people act as if they’re afraid of you. As he explained in a 2016 TEDMED talk, “This scale captures ways in which the dignity and the respect of people who society does not value is chipped away on a daily basis.”
[contentarea class=”bwh-ca”]
Maternal Mortality in the U.S.: A Human Rights Crisis
Despite high-tech medical advances of the last century, women around the world are still dying in pregnancy and childbirth from age-old scourges such as hemorrhage and pre-eclampsia and, increasingly, from complications related to chronic diseases, obesity, and advanced maternal age.
In 2000, the global health and development community acknowledged the need for action in Goal 5 of the U.N. Millennium Development Goals, which aimed to reduce maternal deaths by three-quarters in 15 years (it declined by 45 percent). While press and publicity around the push offered harrowing stories, women reading these stories in the U.S. may well have come away believing that it was a problem for mothers in villages in Sierra Leone—but surely not in Atlanta or Washington, D.C.
Starting in 2008, human rights groups around the world began calling on the U.S. to do more to keep its mothers from dying. The United Nations Committee on the Elimination of Racial Discrimination (CERD) expressed concern about inequities in maternal mortality and recommended that steps be taken to improve access to maternal health care, family planning, and sexuality education and information.
A 2012 Amnesty International report declared that these steps weren’t enough: “Preventable maternal mortality can result from or reflect violations of a variety of human rights, including the right to life, the right to freedom from discrimination, and the right to the highest attainable standard of health.” Having ratified two key international treaties guaranteeing these rights, the authors wrote, the U.S. government should be held accountable.
Four years later, representatives from the advocacy organization SisterSong, the Center for Reproductive Rights, and National Latina Institute for Reproductive Health issued a report to CERD further exploring these issues. CERD adopted the groups’ recommendations, including addressing stereotypes that promote discrimination in clinical settings and standardizing data collection on maternal deaths. In 2015, an advocacy organization called Black Mamas Matter emerged out of this effort to keep pushing the agenda forward.
To the women leading the charge, one central fact was clear: Racism is an undeniable thread running through the stories of black mothers who die. But as Elizabeth Dawes Gay, co-director of Black Mamas Matter and a public health professional, wrote in The Nation, providers and researchers often place “the onus for large-scale change on individuals rather than the systems that we know cause harm.”
[/contentarea]
The telomere connection
In the early 2000s, research on telomeres—protective caps on chromosomes—provided further evidence that weathering is not merely a metaphor but a biological reality. Each time cells divide, telomeres get a little shorter. They eventually reach a point where they can’t divide anymore and die. Allostatic load causes cells to divide faster to keep repairing themselves. The result is earlier deterioration of organs and tissues—essentially, premature aging.
“This is what I’ve been talking about all along,” Geronimus says. “Weathering is a biological response to social factors—a product of your lived experience and how that impacts you physiologically. But now, I can describe this even more specifically, in terms of physiological mechanisms. The emerging science gives the concept of weathering a kind of substance or credibility, which has allowed more people to be open to it.”
Geronimus has incorporated the study of allostatic load and telomere length into her own work. She recently led a study of telomere length in Detroit among low-income individuals of multiple races and ethnicities. The results suggested that community and kin networks may be more protective for health than income and education.
Indeed, in this study population, poor white individuals actually experienced more weathering than poor minority populations, and Hispanics with more education experienced more weathering than those with less education. Social isolation and feeling estranged from one’s community, whether because of occupational or educational differences, along with everyday exposure to discrimination in new, predominantly white, middle-class contexts—in popular lingo, being “othered”—may explain these outcomes, Geronimus says.
She hopes to dig further into this line of inquiry, to find out which social stressors matter the most for health, how they can be disrupted, and how the scientific findings can be turned into policy. “If someone is experiencing weathering because of the discrimination they face in their lives,” she says, “the solution is not just to tell them to get more exercise.”
That Geronimus’ ideas have become mainstream in the field was evident at the 23rd Annual HeLa Women’s Health Symposium, held in September 2018 at Morehouse School of Medicine, in Atlanta. This year’s event focused on maternal health disparities, and Geronimus’ findings bubbled up in the talks of many speakers. Researchers and advocates said that a key part of reducing maternal deaths was addressing the societal conditions that affect women’s health throughout their lives, like housing, air quality, and nutrition. One of those speakers was a fellow Harvard Chan alumna and a public health professional who was in a position to make a difference.
Finding stories in statistics
When she was growing up in a military family in California’s San Fernando Valley, Wanda Barfield, MPH ’90, a rear admiral in the U.S. Public Health Service and director of the Division of Reproductive Health at the CDC, was the kind of kid who would tend to an injured squirrel that fell out of a palm tree. She could never turn away a creature in distress, she says, and often had a stray dog or cat at home under her care. Veterinary medicine seemed like an obvious career path, but as an undergraduate at the University of California–Irvine, she learned about another vulnerable population in need of her big heart.

Wanda Barfield, MPH ’90, director of the Division of Reproductive Health, U.S. Centers for Disease Control and Prevention
Black babies were twice as likely to die within their first year as white babies, Barfield read in the Heckler Report. That insight was life-changing.
Barfield, who is African American, had grown up largely protected from the harsh realities of U.S. health inequities. Her dad was in the Navy’s submarine service, a job that came with secure housing and high-quality, accessible health care for his family. Reading the government report completely altered her perspective, and volunteering in a neonatal intensive care unit (NICU) sealed the deal. “I knew I wanted to care for babies and somehow close the gap,” she says. “As I started learning more about working in the NICU, I realized that a baby’s health is related to the health of the mother, and that the health of the mother is related to her community and to the circumstances of her life. I learned that the social determinants of health mattered in very real and concrete ways.”
Barfield entered Harvard Medical School in 1985, one of just 24 students selected to participate in a new approach to medical education focused on problem solving and early patient interaction. Encouraged to take time off before her last year of medical school to earn an MPH at the Harvard Chan School, Barfield researched infant health outcomes in military families. Overall, African American babies in this population were healthier compared with babies in the general African American population, and their birth weights were higher.
One factor that may have made a difference: better access to care, which included more frequent prenatal visits. But Barfield notes that access is just a small piece of the overall health care women receive. More women are going into pregnancy with diabetes, hypertension, and overweight, she says, and these can threaten pregnancy.
But health care is not just a matter of scheduling an appointment. Mary Wesley, DrPH ’18, an epidemiologist and health services consultant working with the Mississippi State Department of Health, organized data from a series of focus groups held with mothers across the state in 2013. Some women reported that they avoided prenatal care because of the way they were treated by providers. These women, many of whom were low-income or lived in rural areas, wanted more education about caring for themselves and their babies but were limited in their choice of providers. If they felt disrespected or unheard in the examining room, there was nowhere else to go.
The CDC currently collects the death certificates of all women who died during pregnancy or within a year of pregnancy. The information is voluntarily provided by the health departments in all 50 states, New York City, and Washington, D.C. But the information is limited, and there is no national standard.
Barfield and others in the field are pushing for wider adoption of Maternal Mortality Review Committees (MMRCs), now operating in about 30 states. Every time a mother dies, these volunteer expert panels meet to review official data as well as other information about the mother’s life, such as media stories or her social media postings. The goal is to identify what went wrong and to develop guidelines for action. In Georgia, for example, where the country’s maternal death rates are highest, the committee has found records of women who developed hypertension during pregnancy and didn’t receive medication soon enough, women who died waiting for unavailable ambulances, and women whose providers didn’t understand warning signs that led to a hemorrhage, just to name a few gaps in the system. “We need these stories to save women’s lives,” Barfield says.
Data that Barfield and her colleagues at the CDC are gathering through a new system called MMRIA (Maternal Mortality Review Information Application)—pronounced “Maria”—may help identify other under-recognized barriers to safe delivery. MMRIA pulls stories together and looks for trends. In its first report, published in January 2018, data from nine states found that the reasons women died varied by race. White mothers were less likely to have died from pre-eclampsia than black mothers, and more likely to have died from mental health issues, including postpartum depression and drug addiction. Barfield hopes to find out whether these results are true across a broader population and is working on expanding the system. Ideally, MMRCs will amass more fine-grained information about the conditions of lost mothers’ lives, so that researchers can understand how to stop these untimely, heartbreaking—and largely preventable—deaths.
“A maternal death is more than just a number or part of a count,” says Barfield. “It is a tragedy that leaves a hole in a family. It is a story that often includes missed opportunities, both inside and outside of the hospital. It’s important to find out why women are dying so we can prevent the circumstances leading to their death.”
[contentarea class=”bwh-ca”]
The Black Women’s Health Study
Every two years, participants in the Black Women’s Health Study (BWHS), an ongoing cohort study of 59,000 black women, are sent questions about their health, their habits, and various experiences in their lives. Some of the questions, including several from the Everyday Discrimination Scale (developed by the Harvard Chan School’s David Williams, see page 20), have focused on their perceptions of the discrimination they experience. Now in its 23rd year, the BWHS is the largest cohort study focused on black women’s health.
The study was launched by Harvard Chan School alumnae Julie Palmer, ScD ’88, and Lynn Rosenberg, SM ’72, ScD ’78, both professors at the Slone Epidemiology Center of Boston University. Noting that the scientifically productive Nurses’ Health Studies included mostly white women, they felt it was important to gather similarly robust data on the health of African American women.
It took a few years before funding agencies were on board. “They weren’t convinced of the value of a study that only included black women and didn’t have a comparison group,” Palmer says. “But we wanted the whole study population to be black women so that we would have as much statistical power as possible. We wanted to study exposure and disease relationships in black women, rather than using resources for a comparison with white women.”
With the National Cancer Institute as a major sponsor, breast cancer emerged as an early area of focus. Researchers already recognized that while black women and white women have a similar chance of developing breast cancer, black women are 40 percent more likely to die from the disease. Today, they know that black women are more likely than white women to develop the most aggressive and less treatment-responsive form of breast cancer, known as estrogen-receptor-negative, or ER-. Exactly why remains a burning question and is being addressed in BWHS research. Palmer led a collaborative analysis of pregnancy data from the BWHS and three other large studies of breast cancer, finding that childbearing without breastfeeding leads to an increased risk of ER- breast cancer. For complicated reasons, breastfeeding is markedly less common among black mothers in the U.S. than in other mothers.
In a line of research separate from BWHS, Nancy Krieger, professor of social epidemiology at the Harvard Chan School, found that early-life exposure to Jim Crow laws—which legalized racial discrimination in Southern U.S. states from the late 1870s through the mid-1960s—was associated with negative health effects decades later. Among U.S. women currently diagnosed with breast cancer, being born in a Jim Crow state raised black women’s risk of being diagnosed with ER- breast tumors.
BWHS investigators are also exploring other conditions that are uncommon in the general population but have emerged in striking numbers in black women, including sarcoidosis, a connective tissue disorder. “We didn’t ask about it; none of us had heard of it,” Palmer says. “On the first questionnaire, we had two write-in spots for other conditions, and a few hundred women wrote in sarcoidosis.” A literature search showed it was more common in blacks than whites and in women than men. One researcher, Yvette Cozier, has made it one of her primary areas of investigation. As Palmer says, “That wouldn’t have happened without 59,000 black women telling us about their health concerns.”
She adds that an African American student working on the study had a preterm birth around the same time that several white women on the team had normal births. The team had already been looking into the effects of discrimination on health—but the student’s unsettling experience was a striking reminder of why the research is important.
[/contentarea]
Saving mothers
Will this growing body of data attesting to black women’s increased risk of death during and after childbirth shape policymaking? Researchers want to see a broad range of changes in health care culture, in public health information gathering, and in society at large. As Neel Shah and Boston University’s Eugene Declercq noted in an August 2018 editorial in STAT, maternal deaths are a “canary in the coal mine for women’s health.” Shah added in a recent interview: “Efforts by clinicians and hospitals to improve maternity care are essential. But we can’t solve the problem of maternal deaths unless we acknowledge that women’s health isn’t something to be concerned about only during pregnancy and then disregarded after the baby is born.”
In 2017, Shah started a national March for Moms to raise public awareness around maternal health. Through his work with Ariadne Labs, he is piloting new approaches to the birth process that ensure that mothers are empowered to make decisions about their care, including a labor and delivery planning whiteboard that helps track mothers’ preferences, health conditions, and birth progress. He says that work is under way on a program to improve community support for mothers during the critical first year after childbirth by galvanizing city governments to coordinate and develop resources.
Along similar lines, the Mississippi State Department of Health offers programs that address issues of quality in care that moms referred to in the focus group discussions, says Mary Wesley. One example is the department’s Perinatal High Risk Management/Infant Services System, a multidisciplinary case management program for Medicaid-eligible, high-risk pregnant and postpartum women and their babies less than 1 year old. The program includes enhanced services with home visits, health education, and psychosocial support for nutritional and mental health needs.
Arline Geronimus takes a wider view of the issue, arguing that the solution to racial inequities in maternal mortality is to change the way society works. In the near term, she says, race should regularly be taken into consideration during prenatal risk screenings, because even younger black women could be at increased risk of pregnancy complications. Risk status by maternal age should be reappraised in context, as well. While most women in their 20s and early 30s are considered low-risk, black women may be weathered and biologically older than their chronological age, she said, which makes them more subject to health complications at younger ages.
This is true even among highly educated or professional women, such as Serena Williams or Shalon Irving. The danger of failing to recognize the effects of weathering in black women of higher socioeconomic position can be compounded. That’s because the U.S. lacks policies that support women who want both careers and parenthood, a gap that can lead professional women to postpone childbearing until their late 30s or 40s. According to Geronimus, “As a group, black mothers in their mid- to late 30s have five times the maternal mortality rate of black teen mothers, although the older mothers generally have greater educational or economic resources and access to health care.”
Ana Langer, professor of the practice of public health and coordinator of the School’s Women and Health Initiative, points out that the 2010 Amnesty International report Deadly Delivery: The Maternal Health Care Crisis in the USA, contained a shocking fact: Most women in the U.S. weren’t dying during childbirth because of the complexity of their health conditions, but because of the barriers they faced in accessing high-quality maternal care—particularly those who were poor or faced racial discrimination.
Video: Black moms share their stories
In general, maternal mortality in the U.S. receives scant attention, Langer adds, in part because there are relatively few deaths each year compared with other conditions, and also because there are no important business opportunities related to conditions that don’t require sophisticated drugs or technologies. But she bluntly suggests an additional reason: “Women—particularly those who are most vulnerable due to their race, age, or socioeconomic status—receive less attention overall for their health issues, compared to men. On a positive note, the attention on gender and sex gaps and social determinants of health in research and care is rapidly increasing. This is the time to build on this growing momentum to increase the efforts to improve maternal health in the U.S.”
In an April 2018 Rewire News story, Elizabeth Dawes Gay, of Black Mamas Matter, directly addressed the racial disparities element in maternal mortality: “Those of us who want to stop black mamas from dying unnecessarily have to name racism as an important factor in black maternal health outcomes and address it through strategic policy change and culture shifts. This requires us to step outside of a framework that only looks at health care and consider the full scope of factors and policies that influence the black American experience. It requires us to examine and dismantle oppressive and discriminatory policies. And it requires us to acknowledge black people as fully human and deserving of fair and equal treatment and act on that belief.”
As Linda Blount, of the Black Women’s Health Imperative, noted during the Morehouse symposium, “Race is not a risk factor. It is the lived experience of being a black woman in this society that is the risk factor.”
Serena Williams understands that. She told the BBC that she had received excellent care overall for her postpartum complications. But then she pulled back the lens. “Imagine all the other women,” she said, who “go through that without the same health care, without the same response.”
Amy Roeder is associate editor of Harvard Public Health.
Photos: Getty Images, Becky Harlan/NPR, Brian Lillie/University of Michigan, U.S. Centers for Disease Control and Prevention
Illustrations: Benjamin S. Wallace/Harvard Chan School